This week I learned that Amazon is now selling more e-books than hardbacks. This can’t be good news for the a(actual)-book business, and may signal the eventual end of the local bookstore. Time will tell. Did I mention that one of my favorite things is to browse around in bookstores? Yesterday that was my errand, and I soon found myself in the Health section. It wasn’t hard because they had a sign hanging from the ceiling, marking the section’s location. That sign seemed larger than similar signs throughout the store, but perhaps this was only an illusion. I discovered that most of the section was an illusion.
The first subsection I came to was “self-improvement.” This had a curious mix of titles and topics, and it wasn’t clear what rules governed what books were included and what books were shelved elsewhere or not at all. There were two notable finds in the section. The first was called “Tai Chi for Dummies.” Here is my question. Who else would read such a book? The second find was a series called FU books, for example “FU job.” I’m not making this up. Apparently this is self-improvement because readers are given permission to release their suppressed hostility and frustration. I suppose it is cheaper than therapy?
The other main health subsection is diet. I wonder what it says about Americans that a small bookstore has 500 titles on how to eat? Is it really that complicated? Perhaps the salvation of bookstores will come from the Health sections. As we get fatter and fatter, we will rush to Barnes & Noble to buy more diet books? Maybe that’s a new diet idea: walk to the bookstore to buy a diet book.
And speaking of diet books, there is a crazy quilt of titles. Here are some of the more captivating: The ABC Diet; The Belly Fat Diet; Biggest Loser (a multiple title series); Change Your Brain, Change Your Body; The Eat Clean Diet; The 5 Factor Diet; The Flat Belly Diet; Get Fit and Live; The GI Diet (go to Afghanistan and eat K rations); How to Never Look Fat Again; I Can Do This Diet; The Kind Diet; Look Better Naked (Really?); Muscle Chow; The Perfect 10 Diet; The Secrets of Skinny Chicks; Skinny Bitch and its companion Skinny Bastard; This is Why You Are Fat; The Thyroid Solution; and You, On a Diet. Of course the old standbys, The Adkins Diet and The South Beach Diet were there. I noticed The Complete Beck Diet; you burn calories by yelling at Obama on YouTube for 30 minutes a day. I also thought it ironic that the diet section has shelves labeled for oversized books!
This set of material defines confusion. Book stores operate on a business plan to move books by the cash register. If the “health” books were not doing that, they wouldn’t be given shelf space. The health literacy level of many people is not up to the task of sorting the wheat from the chaff among and within these books. Here there is also a metaphor for the U.S. market-driven health care system. Those who despise government’s participation in health care decisions believe that bureaucrats will interfere with what is best by getting in between us and our physicians. However, unfettered market driven health care is like market driven health books on a grand scale.
As I was leaving the store I wanted to change the section sign to read “Health, sort of.”
Friday, July 30, 2010
Thursday, July 29, 2010
Ready and Smart
Health promotion is mostly linked to primary prevention - things to do to protect health in the first place, avoiding the development of illness or injury. Further, the term is often associated with lifestyle habits such as diet, exercise, stress management, avoiding smoking, and so forth. In the late 1990s, and accelerating after 9/11, health promoters have increasingly become engaged in what has come to be called emergency preparedness. Of course there have been hospital emergency departments and ambulance services for decades, but the more recent concept of emergency preparedness encompasses an array of threats, including natural disasters, infectious disease outbreaks, such as pandemic flu, and ever more hideous manifestations of terrorism. While emergency preparedness incorporates much more than health promotion, it has a role to play as we try to assure people have the best health possible in the face of the worst that nature and mankind can throw at them.
Preparedness is challenging for many reasons. For one thing, we try to be prepared for any emergency. Not long ago I worked on a team with school systems in a project to build their preparedness. A first step was for schools to identify any particular threats beyond the universal ones like severe weather or a shooter. One school system was down river from a dam showing signs of breakdown. Making repairs on the dam was a multi-year process, and until completed, persons and buildings below were at risk. If the dam failed, students would have to be bused out of harm’s way. Another system had schools in the flight path of a major airport while another school system was in a terrorism target zone near a major military base. Such a broad range of potential emergencies means that there is no universal preparedness template. Every community needs a unique plan.
Another reason emergency preparedness is challenging is because the key participants don’t have routine established patterns of working together. For example, if there was a serious bomb threat at a public school, the community response would need to include principal, superintendent, teachers, parents, police and fire departments, emergency medical services, news media, health care system, and local government. These players do not routinely work together. They don’t have integrated dispatch and communication systems. There is no obvious way to organize so that everyone knows what to do and who is in charge. Many communities have designed and practiced emergency plans, but it is very difficult to maintain the ability to spring into action according to the plan. Federal and state units of homeland security have worked hard to enhance community readiness. Most officials believe we are better prepared than we were 10 years ago, but no one really wants to put it to the test.
In addition to the primary response to community crises, there is also the consideration of mental health implications for responders and residents. Depending on the circumstances of an emergency, often the response workforce as well as immediate victims and community residents are emotionally traumatized. If the situation arises where hundreds or thousands of people experience extreme stress and anxiety, the mental health system is asked to find a way to respond to a sudden surge of clients. This also has to be part of a response plan.
The work of community preparedness illustrates how interdisciplinary the worked has become. Planning has gone beyond first responders to include new participants, such as engineers. Engineering tools and techniques are used to guide resource flow and organizational dynamics. Computerized expert systems are being harnessed to guide contingency flow charts in response to varying threats and circumstances. The skill set needed to respond in complex circumstances is found in a wider and wider range of professional expertise.
In the Spanish language, there is a common phrase “Estoy listo,” which means “I am ready” or “Estan listo?” “Are you ready?” Spanish speakers will also use listo to mean smart -“Este chico es listo,” “That boy is smart.” In emergency preparedness we have to be both ready and smart.
Preparedness is challenging for many reasons. For one thing, we try to be prepared for any emergency. Not long ago I worked on a team with school systems in a project to build their preparedness. A first step was for schools to identify any particular threats beyond the universal ones like severe weather or a shooter. One school system was down river from a dam showing signs of breakdown. Making repairs on the dam was a multi-year process, and until completed, persons and buildings below were at risk. If the dam failed, students would have to be bused out of harm’s way. Another system had schools in the flight path of a major airport while another school system was in a terrorism target zone near a major military base. Such a broad range of potential emergencies means that there is no universal preparedness template. Every community needs a unique plan.
Another reason emergency preparedness is challenging is because the key participants don’t have routine established patterns of working together. For example, if there was a serious bomb threat at a public school, the community response would need to include principal, superintendent, teachers, parents, police and fire departments, emergency medical services, news media, health care system, and local government. These players do not routinely work together. They don’t have integrated dispatch and communication systems. There is no obvious way to organize so that everyone knows what to do and who is in charge. Many communities have designed and practiced emergency plans, but it is very difficult to maintain the ability to spring into action according to the plan. Federal and state units of homeland security have worked hard to enhance community readiness. Most officials believe we are better prepared than we were 10 years ago, but no one really wants to put it to the test.
In addition to the primary response to community crises, there is also the consideration of mental health implications for responders and residents. Depending on the circumstances of an emergency, often the response workforce as well as immediate victims and community residents are emotionally traumatized. If the situation arises where hundreds or thousands of people experience extreme stress and anxiety, the mental health system is asked to find a way to respond to a sudden surge of clients. This also has to be part of a response plan.
The work of community preparedness illustrates how interdisciplinary the worked has become. Planning has gone beyond first responders to include new participants, such as engineers. Engineering tools and techniques are used to guide resource flow and organizational dynamics. Computerized expert systems are being harnessed to guide contingency flow charts in response to varying threats and circumstances. The skill set needed to respond in complex circumstances is found in a wider and wider range of professional expertise.
In the Spanish language, there is a common phrase “Estoy listo,” which means “I am ready” or “Estan listo?” “Are you ready?” Spanish speakers will also use listo to mean smart -“Este chico es listo,” “That boy is smart.” In emergency preparedness we have to be both ready and smart.
Wednesday, July 28, 2010
Disability in America
This week marks the 20th anniversary of the passage of the federal Americans with Disabilities Act. Depending on your point of view, the law is a satisfying advancement for social justice or a notorious example of government overreach causing wasteful spending of tax dollars and intrusion into private property rights. It is all a matter of perspective.
When I was young, we had no one with a disability. No, I didn't live in Lake Woebegon ("all the women are strong, all the men are good looking, and all the children are above average"). It was just that people out of the mainstream were hidden away, shut out from common activities and events. If you were paralyzed or deaf, that was sad, but you were supposed to be out of sight in a specialized institution, not making the rest of us morose or inconvenienced. It was more true then, that people were defined by their limitation: they were "the blind" as opposed to a friend, a parent, a classmate who happened to have a vision impairment.
This was all changed with the passage of the Americans With Disabilities Act, passed by Congress (only 8 Senators and 28 Congressmen voted against) in 1989 and signed by President Bush in 1990. This was a landmark change of course for our treatment of people with disabilities and a model of American exceptionalism for the world. Some of the most recognized provisions are banning employment discrimination against those with disabilities, making sure all people are able to use public accommodations, with measures such as curb cuts, entry ramps, accessible public bathrooms, devices and technology for those with hearing problems, handicapped parking, and school services to assure equal opportunity for those with special needs.
The regulations stemming from the bill's precepts are still unfolding and evolving. For example, court cases have established that infectious disease ( e.g. HIV/AIDS) and mental illness can be considered disabilities, giving discrimination protection to those effected. As the scientific understanding of obesity proliferates, it is becoming apparent that body weight is not just a function of choices regarding eating and exercise, but that there are powerful physiological mechanisms playing a role, and that these mechanisms are not under voluntary control. Time will tell whether we will recognize that overweight people have unique civil rights concerns that should be protected by ADA rules.
Even before passage of ADA, there was a series of federal court cases dealing with disability discrimination in various settings and circumstances. The history of those cases shows an evolving consensus on the Court, from a starting point of strong doubts about the standing of disability as worthy of civil rights protections, but after relentless educating by disability advocates, the justices began to understand. As an aside, this is support for Obama's assertion that empathy is a useful trait for Supreme Court judges. In this case, judicial empathy grew as judges became better informed.
From time to time I ride a public bus to work. The bus has the capability to lower the entrance to the level of the side walk, to facilitate entrance by a person in a wheel chair. It also helps for someone pulling a suit case or cart with wheels. The entrance is wider than was true in years past, again to accommodate wheel chairs. Within the bus, there is a section of seats which fold up, revealing devices to secure a wheel chair to the bus, making it possible for people to ride safely. The stop cord is designed so that someone sitting low in a wheel chair is able to request the driver to stop at the next corner. On that same bus I see people guided by seeing eye dogs, and though I haven't seen this, the bus could also accommodate someone with a "hearing" dog. Finally, I also see mentally handicapped persons accompanied by a guide, helping them get to their destination. All of these provisions cost tax dollars. It is probably more efficient to just put people in institutions. But how much does our society gain by full, or almost full participation? Is Congress a better decision-making body because we have Jim Langevin serving, the first quadriplegic U.S. Congressman. The answer is most certainly yes.
Disability is related to health promotion in one important way. Both are about doing more and stretching limits. What is the limit on how far someone with a disability can overcome? In a similar way, what is possible with health improvement? Good health is a moving target; no matter where you are, it can always be better. You can never be so healthy that you can't be more so.
Some years ago, I first saw a group of blind skiers threading their way down a Colorado ski slope. It was nothing short of inspirational, and taught me that health truly is for all, that health promotion must be tailored for an individual’s needs, and anything is possible.
When I was young, we had no one with a disability. No, I didn't live in Lake Woebegon ("all the women are strong, all the men are good looking, and all the children are above average"). It was just that people out of the mainstream were hidden away, shut out from common activities and events. If you were paralyzed or deaf, that was sad, but you were supposed to be out of sight in a specialized institution, not making the rest of us morose or inconvenienced. It was more true then, that people were defined by their limitation: they were "the blind" as opposed to a friend, a parent, a classmate who happened to have a vision impairment.
This was all changed with the passage of the Americans With Disabilities Act, passed by Congress (only 8 Senators and 28 Congressmen voted against) in 1989 and signed by President Bush in 1990. This was a landmark change of course for our treatment of people with disabilities and a model of American exceptionalism for the world. Some of the most recognized provisions are banning employment discrimination against those with disabilities, making sure all people are able to use public accommodations, with measures such as curb cuts, entry ramps, accessible public bathrooms, devices and technology for those with hearing problems, handicapped parking, and school services to assure equal opportunity for those with special needs.
The regulations stemming from the bill's precepts are still unfolding and evolving. For example, court cases have established that infectious disease ( e.g. HIV/AIDS) and mental illness can be considered disabilities, giving discrimination protection to those effected. As the scientific understanding of obesity proliferates, it is becoming apparent that body weight is not just a function of choices regarding eating and exercise, but that there are powerful physiological mechanisms playing a role, and that these mechanisms are not under voluntary control. Time will tell whether we will recognize that overweight people have unique civil rights concerns that should be protected by ADA rules.
Even before passage of ADA, there was a series of federal court cases dealing with disability discrimination in various settings and circumstances. The history of those cases shows an evolving consensus on the Court, from a starting point of strong doubts about the standing of disability as worthy of civil rights protections, but after relentless educating by disability advocates, the justices began to understand. As an aside, this is support for Obama's assertion that empathy is a useful trait for Supreme Court judges. In this case, judicial empathy grew as judges became better informed.
From time to time I ride a public bus to work. The bus has the capability to lower the entrance to the level of the side walk, to facilitate entrance by a person in a wheel chair. It also helps for someone pulling a suit case or cart with wheels. The entrance is wider than was true in years past, again to accommodate wheel chairs. Within the bus, there is a section of seats which fold up, revealing devices to secure a wheel chair to the bus, making it possible for people to ride safely. The stop cord is designed so that someone sitting low in a wheel chair is able to request the driver to stop at the next corner. On that same bus I see people guided by seeing eye dogs, and though I haven't seen this, the bus could also accommodate someone with a "hearing" dog. Finally, I also see mentally handicapped persons accompanied by a guide, helping them get to their destination. All of these provisions cost tax dollars. It is probably more efficient to just put people in institutions. But how much does our society gain by full, or almost full participation? Is Congress a better decision-making body because we have Jim Langevin serving, the first quadriplegic U.S. Congressman. The answer is most certainly yes.
Disability is related to health promotion in one important way. Both are about doing more and stretching limits. What is the limit on how far someone with a disability can overcome? In a similar way, what is possible with health improvement? Good health is a moving target; no matter where you are, it can always be better. You can never be so healthy that you can't be more so.
Some years ago, I first saw a group of blind skiers threading their way down a Colorado ski slope. It was nothing short of inspirational, and taught me that health truly is for all, that health promotion must be tailored for an individual’s needs, and anything is possible.
Tuesday, July 27, 2010
Healthy Cities Rankings
There is something about human nature that makes us want to compare ourselves with others. When I was in school I used to hate it when classmates would ask what I got on the test, but I was guilty of doing it as well. An extension of this tendency is that we even compare things in which we are involved only indirectly or not at all. We compare the best and worst dressed celebrities, the most attractive rag top autos, the best beaches. This is an indoor sport for many people, and makes for pleasant off the clock chatter.
Among all the types of comparisons and list making, rankings of the healthiest places to live appear in the media or online from time to time. Like all listings and rankings, identifying the most and least healthy places is an inexact science, to say the least. The label "healthiest city" is not valid because there is no universal standard. In fact, there are several different lists, and each one defines and measures "healthiest" in different ways. It may include death rates, infant death rates, rates of hospitalization and average length of stay in hospitals, the proportion of people who smoke, the median body mass index (BMI) as an indicator of prevailing overweight and obesity, number of people for each physician, dentist, and mental health counselor, miles of bike lanes per person, and many more considerations. Depending on which variables are included in the determination of healthiest, and how those variables are weighted, the ranking will vary greatly for the same city.
The rankings don't explain why a city is high or low on the list. For example, the city of Louisville ranks low on at least one listing, due to a high smoking rate, compared to many other communities. The ranking doesn’t explain why there is so much smoking here. On the other hand, New Orleans also ranks low, in part because its infrastructure is crumbling, due to poverty, disruption of community services stemming from Hurricane Katrina, and now the economic turmoil caused by the BP oil spill. While Louisville’s ranking is low, it is not a reason for someone to not want to live there because the smoking mostly effects smokers. On the other hand, the problems in New Orleans effect all residents. Rankings should be probed to understand what they mean to present or potential residents.
Within each city there is a great diversity in health status between individuals. Individual level health status tracks with education, income, housing and neighborhood qualities, as well as personal lifestyle habits. Even in places judged to be unhealthy over all will have some very healthy persons. Those cities considered very health will have some people in very poor health. The common rankings don’t adjust for population differences which may be important. For example, because Tampa has a lot of retired, older people, we would expect its health profile to be different than cities like Seattle or Anchorage, AK, which tend to have a much younger population. Somehow it is not quite right to judge Tampa as an unhealthy city, just because of an aging population.
What, then, is the practical value of these rankings. In a broader sense there is good reason to assess a community’s health and well being. This is routine practice in health promotion and public health, so that we take a periodic community pulse to see if progress is being made. It is also useful data to serve as the basis for making program decisions. For example, what health problem deserves the most attention in your neighborhood or community? Is it HIV, childhood asthma, skin cancer, or teen pregnancy? An answer has to be based on data, not just arbitrary choices.
Just the concept of healthiest city implies that we are all connected, and that there are aspects of health which are group concerns. There is a lot about your health which depends on your choices and actions as an individual. For example, you have to decide portion size and what foods you eat. The community can influence but ultimately you decide. To a greater extent than most people realize, your health is also dependent on community decisions and policies which provide circumstances under which all people can thrive. It is not just about me or just about you, it is often about us.
Among all the types of comparisons and list making, rankings of the healthiest places to live appear in the media or online from time to time. Like all listings and rankings, identifying the most and least healthy places is an inexact science, to say the least. The label "healthiest city" is not valid because there is no universal standard. In fact, there are several different lists, and each one defines and measures "healthiest" in different ways. It may include death rates, infant death rates, rates of hospitalization and average length of stay in hospitals, the proportion of people who smoke, the median body mass index (BMI) as an indicator of prevailing overweight and obesity, number of people for each physician, dentist, and mental health counselor, miles of bike lanes per person, and many more considerations. Depending on which variables are included in the determination of healthiest, and how those variables are weighted, the ranking will vary greatly for the same city.
The rankings don't explain why a city is high or low on the list. For example, the city of Louisville ranks low on at least one listing, due to a high smoking rate, compared to many other communities. The ranking doesn’t explain why there is so much smoking here. On the other hand, New Orleans also ranks low, in part because its infrastructure is crumbling, due to poverty, disruption of community services stemming from Hurricane Katrina, and now the economic turmoil caused by the BP oil spill. While Louisville’s ranking is low, it is not a reason for someone to not want to live there because the smoking mostly effects smokers. On the other hand, the problems in New Orleans effect all residents. Rankings should be probed to understand what they mean to present or potential residents.
Within each city there is a great diversity in health status between individuals. Individual level health status tracks with education, income, housing and neighborhood qualities, as well as personal lifestyle habits. Even in places judged to be unhealthy over all will have some very healthy persons. Those cities considered very health will have some people in very poor health. The common rankings don’t adjust for population differences which may be important. For example, because Tampa has a lot of retired, older people, we would expect its health profile to be different than cities like Seattle or Anchorage, AK, which tend to have a much younger population. Somehow it is not quite right to judge Tampa as an unhealthy city, just because of an aging population.
What, then, is the practical value of these rankings. In a broader sense there is good reason to assess a community’s health and well being. This is routine practice in health promotion and public health, so that we take a periodic community pulse to see if progress is being made. It is also useful data to serve as the basis for making program decisions. For example, what health problem deserves the most attention in your neighborhood or community? Is it HIV, childhood asthma, skin cancer, or teen pregnancy? An answer has to be based on data, not just arbitrary choices.
Just the concept of healthiest city implies that we are all connected, and that there are aspects of health which are group concerns. There is a lot about your health which depends on your choices and actions as an individual. For example, you have to decide portion size and what foods you eat. The community can influence but ultimately you decide. To a greater extent than most people realize, your health is also dependent on community decisions and policies which provide circumstances under which all people can thrive. It is not just about me or just about you, it is often about us.
Monday, July 26, 2010
Health and Literacy
If you are reading this blog, you are like me in the sense that we take reading and vocabulary for granted. This is somewhat like cultural sensitivity. If you are a mainstream majority person, meaning middle class, and reasonably well educated, there is a tendency to not appreciate the challenges faced by people of minority culture who cope with English as a second language. Those in the majority (myself included) are often blind to discrimination. It doesn't happen to us, so we don't see it, especially in more subtle forms.
National surveys of adult literacy have been done in the U.S. since the early 90s. For measurement purposes, literacy is divided into categories. Prose literacy is the ability to read and comprehend passages of sentences and paragraphs. Document literacy is the ability to navigate through non-continuous text, such as a job application or a medical history form. Numeracy is the ability to use simple numbers in every day application, such as figuring a tip at a restaurant or working with numbers in a set of instructions. The other dimension of measurement is levels of proficiency (below basic, basic, intermediate, proficient). As a nation, approximately 14% of adults are significantly limited (below basic) in the various types of literacy, according to the most recent national survey. This translates into millions of people. Of course, limited literacy is clustered in low income, poorly educated, those living in rural communities, minority groups, those whose primary language is not English, and senior citizens. Seniors have twice the prevalence of below basic literacy while at the same time making up a disproportionate share of the patient population. We have also learned that many people whose first language is not English have limited literacy in their own language.
Overlaid on this general problem of limited literacy is the challenge of comprehending health and medical information. Because health information often is expressed in very technical and specialized language, even people who are otherwise well educated have trouble. Not all, but some of the popularity of unfounded alternative treatments and unproven health boosting advice is due to the promoters being able to communicate in clear and compelling ways, whereas people leave their doctor's office scratching their heads.
This is a problem in which everyone is invested. Unless you live in a very rarefied social circle where everyone is well educated and affluent, you know, perhaps without realizing, someone who struggles with understanding medication label instructions or patient education materials about a chronic disease. If you are a health care provider or allied health professional, you may need to examine your manner of speaking and the nature of printed materials you routinely give to patients. The rest of us should care about this because this gap in understanding between patients and health care workers translates into excess illness and death. When someone cannot understand how to take a medication or doesn't comprehend how to follow a therapeutic diet, they run a greater risk of failing to benefit from treatment, failing to control illnesses, and suffering consequences including premature death. This is a human loss, but also an economic one, adding to the already out-of-control cost of our health care system.
The health care system is beginning to respond to this problem. More and more hospitals, physicians and other practitioners, insurers, and nonprofit organizations are trying to be more user-friendly for all consumers. It is a more difficult challenge to bring about community circumstances so that all adults obtain more adequate reading and numerical skills. This illustrates that education reform has wide repercussions.
Note also that improving health literacy, working from both sides, is still only a partial solution. People follow or do not follow health advice for very complex reasons. Information understanding is required, but is not sufficient in itself. Health literacy is a good place to start as the nation continues to push toward health for all.
National surveys of adult literacy have been done in the U.S. since the early 90s. For measurement purposes, literacy is divided into categories. Prose literacy is the ability to read and comprehend passages of sentences and paragraphs. Document literacy is the ability to navigate through non-continuous text, such as a job application or a medical history form. Numeracy is the ability to use simple numbers in every day application, such as figuring a tip at a restaurant or working with numbers in a set of instructions. The other dimension of measurement is levels of proficiency (below basic, basic, intermediate, proficient). As a nation, approximately 14% of adults are significantly limited (below basic) in the various types of literacy, according to the most recent national survey. This translates into millions of people. Of course, limited literacy is clustered in low income, poorly educated, those living in rural communities, minority groups, those whose primary language is not English, and senior citizens. Seniors have twice the prevalence of below basic literacy while at the same time making up a disproportionate share of the patient population. We have also learned that many people whose first language is not English have limited literacy in their own language.
Overlaid on this general problem of limited literacy is the challenge of comprehending health and medical information. Because health information often is expressed in very technical and specialized language, even people who are otherwise well educated have trouble. Not all, but some of the popularity of unfounded alternative treatments and unproven health boosting advice is due to the promoters being able to communicate in clear and compelling ways, whereas people leave their doctor's office scratching their heads.
This is a problem in which everyone is invested. Unless you live in a very rarefied social circle where everyone is well educated and affluent, you know, perhaps without realizing, someone who struggles with understanding medication label instructions or patient education materials about a chronic disease. If you are a health care provider or allied health professional, you may need to examine your manner of speaking and the nature of printed materials you routinely give to patients. The rest of us should care about this because this gap in understanding between patients and health care workers translates into excess illness and death. When someone cannot understand how to take a medication or doesn't comprehend how to follow a therapeutic diet, they run a greater risk of failing to benefit from treatment, failing to control illnesses, and suffering consequences including premature death. This is a human loss, but also an economic one, adding to the already out-of-control cost of our health care system.
The health care system is beginning to respond to this problem. More and more hospitals, physicians and other practitioners, insurers, and nonprofit organizations are trying to be more user-friendly for all consumers. It is a more difficult challenge to bring about community circumstances so that all adults obtain more adequate reading and numerical skills. This illustrates that education reform has wide repercussions.
Note also that improving health literacy, working from both sides, is still only a partial solution. People follow or do not follow health advice for very complex reasons. Information understanding is required, but is not sufficient in itself. Health literacy is a good place to start as the nation continues to push toward health for all.
Friday, July 23, 2010
Exalted Valleys and Low Mountains
In Old Testament scripture there is a passage about preparing the way for one who is to come, exalting valleys and making mountains low. These are, for some, stirring lines that provided lyrics for a section of Handel's Messiah. The passage has an aura of excitement, optimism and hope, lifting the reader out of the dreary and dull. This is a role for all things inspirational, supporting the promotion of health in important ways.
In my part of the world there is a battle of mountains and valleys going on in the coal regions of Appalachia. It is anything but inspirational. I'm talking about mountain top removal as a method of extracting coal from the earth. The method essentially cuts off the top section of those mountains with substantial coal reserves, leaving a flat top barren of topsoil, trees, and wild life. The refuse material, including dirt and plant material is simply pushed over the side, covering the bottom of valleys and filling in creeks and streams. In addition to stealing the natural beauty of the region, the process pollutes the water sources of the nearby communities. Instead of preparing for something which will make life better, this process leaves behind despair and ugly landscape scars. Below are some pictures of the aftermath of mountain top removal. The sources are earthclub.wordpress.com and mountainroadshow.com.


The local people are ambivalent about what is happening to their domain. The coal companies provide jobs where none others exist. Coal mining has been a part of these communities for generations, and yet the health status and standard of living have been stuck on the bottom. They certainly don't like poison in their drinking water and their houses being shaken from the blasting of the coal deposits. The coal companies give back just enough to keep a workforce, but otherwise only care about taking the coal until it is gone. These are companies and managers people find easy to despise, though I'm sure they view themselves as just trying to run a business.
If we respected the land and the people who live in Appalachia, and cut our use of coal for generating electricity, the region would have even more desperate poverty. Less coal would mean less air pollution and less release of greenhouse gases, perhaps slowing down the process of climate change. Unfortunately, until new technology is perfected and proliferates, the only replacement for power generation in most parts of the country is nuclear energy. As of now, the public is afraid of the potential risk. Perhaps that needs to change.
Conservation can help, but the lead time for substantially decreasing power use by consumers and industries is measured in decades.. We are hooked on cheap electricity. By national standards, Kentucky has very low electricity rates; by international standards, the U.S.also has low rates, for example, compared to most European countries. A higher price would accelerate the drive for conservation, like it has done in Europe, but consumers are resistant of anything, such as carbon credits, which might lead to price increases for electricity, and products which depend on it.
Perhaps to most people, this is yesterday's news. I think it does illustrate the contrast between market-based solutions and maximum individual autonomy versus community agreement and solutions. Like all health promotion, there is a community policy component to the issue of energy production and consumption. I think we make more progress with such complex issues if we come together for long term solutions rather than putting premium value on the freedom to be a lone ranger. United we stand is a great idea. What if we actually tried it?
In my part of the world there is a battle of mountains and valleys going on in the coal regions of Appalachia. It is anything but inspirational. I'm talking about mountain top removal as a method of extracting coal from the earth. The method essentially cuts off the top section of those mountains with substantial coal reserves, leaving a flat top barren of topsoil, trees, and wild life. The refuse material, including dirt and plant material is simply pushed over the side, covering the bottom of valleys and filling in creeks and streams. In addition to stealing the natural beauty of the region, the process pollutes the water sources of the nearby communities. Instead of preparing for something which will make life better, this process leaves behind despair and ugly landscape scars. Below are some pictures of the aftermath of mountain top removal. The sources are earthclub.wordpress.com and mountainroadshow.com.


The local people are ambivalent about what is happening to their domain. The coal companies provide jobs where none others exist. Coal mining has been a part of these communities for generations, and yet the health status and standard of living have been stuck on the bottom. They certainly don't like poison in their drinking water and their houses being shaken from the blasting of the coal deposits. The coal companies give back just enough to keep a workforce, but otherwise only care about taking the coal until it is gone. These are companies and managers people find easy to despise, though I'm sure they view themselves as just trying to run a business.
If we respected the land and the people who live in Appalachia, and cut our use of coal for generating electricity, the region would have even more desperate poverty. Less coal would mean less air pollution and less release of greenhouse gases, perhaps slowing down the process of climate change. Unfortunately, until new technology is perfected and proliferates, the only replacement for power generation in most parts of the country is nuclear energy. As of now, the public is afraid of the potential risk. Perhaps that needs to change.
Conservation can help, but the lead time for substantially decreasing power use by consumers and industries is measured in decades.. We are hooked on cheap electricity. By national standards, Kentucky has very low electricity rates; by international standards, the U.S.also has low rates, for example, compared to most European countries. A higher price would accelerate the drive for conservation, like it has done in Europe, but consumers are resistant of anything, such as carbon credits, which might lead to price increases for electricity, and products which depend on it.
Perhaps to most people, this is yesterday's news. I think it does illustrate the contrast between market-based solutions and maximum individual autonomy versus community agreement and solutions. Like all health promotion, there is a community policy component to the issue of energy production and consumption. I think we make more progress with such complex issues if we come together for long term solutions rather than putting premium value on the freedom to be a lone ranger. United we stand is a great idea. What if we actually tried it?
Wednesday, July 21, 2010
Whose Role Model Are You?
Sometime in ancient history a wise one made the observation that humans influence each other inadvertently. Children mimic older children and adults. Adults mimic other adults who they admire. In a sense, we are all someone’s rock star, though more often than not, the interpersonal influence is not intentional or even fully conscious. In the 20th century this insight took on formal credibility as a number of social science researchers, such as Albert Bandura and his Social Learning Theory, applied research designs to measure and test how we influence one another. This construct became known as observational learning, or more popularly, role modeling.
Role modeling is just part of the ecology: we influence and are influenced by each other, just like acorns fall down from trees and spring follows winter in temperate climates. Even other animals demonstrate observational learning between generations. The natural progression is to not just recognize but to engineer observational learning. The idea is to harness interpersonal influence for individual or public good. This is one of the most widely used techniques in health promotion. We try to teach parents to be better examples for their children, with respect to smoking, diet, exercise, safety, and so forth. Another approach is to use older students to influence younger ones. Often the cachet of athletes is exploited for this purpose.
It gets more sensitive when role modeling is based on specific individuals because we are all multidimensional. Barack Obama is a good role model because he publicly exercises and stays trim. On the other hand he smokes, though to his credit, he’s made this very private behavior. Lindsey Lohan could be a good role model if she was willing. She certainly has a platform, and has numerous qualities thought desirable by many teens. She hasn’t actively chosen to be a bad role model, but only to succumb to her own destructive patterns.
Some years ago I heard a radio interview with Frank Shorter, who was a very well known long distance runner in the 60s and 70s, winning a gold and silver medal in the Olympic marathon in 1972 and 1976, respectively. At the time of the interview he was still running competitively. The radio host, admiring his muscle stamina and cardiovascular endurance, asked him about his diet. My first thought was, “Oh great, he can give a personal testimony for whole grains, fruits and vegetables.” Turned out he ate mostly junk food and beer. We didn’t make him a poster boy for health and wellness!
Clergy could be important health role models because they play a central leadership role in many communities and congregations. Because they function as first responders for all kinds of life events, they have many opportunities to be sources of constructive observational learning. Unfortunately, evidence shows that as a group (see Clergy Health Initiative), they are not particularly healthy. Among their ranks, overweight is more common than in their non-clergy peers, and the prevalence of many chronic diseases is higher. They are in a position to be positive role models, and are often sought out by health promotion advocates to take on that role, but there are obviously some obstacles.
What if you don’t want to be a role model? Can leaders put boundaries around themselves? Leadership (starting with parent leaders) usually means people will intrude on your privacy. Is your example something you can titrate, measuring out how much and when it is released? I don’t think we can. We can choose to be better or worse, and there is a scientific approach to coaching people to be better role models. Some people are unwilling or just unsuited to be health examples.
Using role modeling as a health promotion technique is in opposition to the more extreme views of independence and libertarianism. “Don’t tread on me!” can also mean “I take no responsibility for what people learn from me. It is not my fault if someone is making bad choices, just because they see me do it.” If you identify with a community approach to making life better, observational learning resonates. If you think everyone should just mind their own business, not so much.
Who is watching you? You can be a health promotion advocate by your example. Or maybe not.
Role modeling is just part of the ecology: we influence and are influenced by each other, just like acorns fall down from trees and spring follows winter in temperate climates. Even other animals demonstrate observational learning between generations. The natural progression is to not just recognize but to engineer observational learning. The idea is to harness interpersonal influence for individual or public good. This is one of the most widely used techniques in health promotion. We try to teach parents to be better examples for their children, with respect to smoking, diet, exercise, safety, and so forth. Another approach is to use older students to influence younger ones. Often the cachet of athletes is exploited for this purpose.
It gets more sensitive when role modeling is based on specific individuals because we are all multidimensional. Barack Obama is a good role model because he publicly exercises and stays trim. On the other hand he smokes, though to his credit, he’s made this very private behavior. Lindsey Lohan could be a good role model if she was willing. She certainly has a platform, and has numerous qualities thought desirable by many teens. She hasn’t actively chosen to be a bad role model, but only to succumb to her own destructive patterns.
Some years ago I heard a radio interview with Frank Shorter, who was a very well known long distance runner in the 60s and 70s, winning a gold and silver medal in the Olympic marathon in 1972 and 1976, respectively. At the time of the interview he was still running competitively. The radio host, admiring his muscle stamina and cardiovascular endurance, asked him about his diet. My first thought was, “Oh great, he can give a personal testimony for whole grains, fruits and vegetables.” Turned out he ate mostly junk food and beer. We didn’t make him a poster boy for health and wellness!
Clergy could be important health role models because they play a central leadership role in many communities and congregations. Because they function as first responders for all kinds of life events, they have many opportunities to be sources of constructive observational learning. Unfortunately, evidence shows that as a group (see Clergy Health Initiative), they are not particularly healthy. Among their ranks, overweight is more common than in their non-clergy peers, and the prevalence of many chronic diseases is higher. They are in a position to be positive role models, and are often sought out by health promotion advocates to take on that role, but there are obviously some obstacles.
What if you don’t want to be a role model? Can leaders put boundaries around themselves? Leadership (starting with parent leaders) usually means people will intrude on your privacy. Is your example something you can titrate, measuring out how much and when it is released? I don’t think we can. We can choose to be better or worse, and there is a scientific approach to coaching people to be better role models. Some people are unwilling or just unsuited to be health examples.
Using role modeling as a health promotion technique is in opposition to the more extreme views of independence and libertarianism. “Don’t tread on me!” can also mean “I take no responsibility for what people learn from me. It is not my fault if someone is making bad choices, just because they see me do it.” If you identify with a community approach to making life better, observational learning resonates. If you think everyone should just mind their own business, not so much.
Who is watching you? You can be a health promotion advocate by your example. Or maybe not.
Tuesday, July 20, 2010
Drug Abuse Doldrums
For most of my now upper middle-aged life, there has been a war on drugs in this country. It has been book-marked by a war on poverty and a war on terror. None has really worked out. Maybe we should declare a war on wars, except for the old fashioned kind - boots on the ground, shoot when you see the whites of their eyes. President Obama has hardly mentioned drug abuse of the illegal version, except perhaps the drug battles spilling over the border from Mexico. He certainly hasn't spent any time talking about what I think is our biggest drug problem, alcohol abuse. And, he is not a champion for reducing tobacco consumption because he seems to struggle with a smoking addiction himself.
I don't necessarily fault him for this silence. The nation is preoccupied by fairly daunting challenges: two wars, near collapse of the financial system, high unemployment, a dysfunctional Congress, a petro fouling of the Mexican Gulf, 13 million illegal aliens, and continuing threats to national security from terrorist organizations. In addition, the President has to walk the dog and check the kids’ homework. All in a day’s work when you are the leader of the free world. While the toll taken by drug abuse has continued unabated, other problems have taken on greater importance and garner more of the nation’s attention.
However, I think there is something else going on. A couple of decades back, the firm resolve of presidents and PTA officers in the face of the “menace” of drugs was accompanied by great optimism. People believed that drugs could be stopped. With enough grit, energy, and investment, we would have drug-free schools and communities. After all, the U.S. wins wars, and we will win this one as well. Forty years in, people have become cynical and burned out. So many programs have been ineffective, and billions of dollars have been spent, with good intentions, but with no results. Abuse of alcohol, tobacco, and other drugs has waxed and waned, but the trends have been mostly unrelated to what governments and community groups have been doing to bend the consumption curve.
From time to time, people ask me what works in drug abuse prevention. “Works” is a loaded word, because it implies that there is something which might really have a huge impact on adolescent and adult drug abuse. Would that were true. In fact, our only chance of bringing about a less drugged citizenry is a combination of small initiatives, none of which makes much difference by itself, but as a package has some promise. This is not being done in any substantial way, but instead we rely on school-based education, which is mostly ineffective, and we put people in jail, which has mostly made these problems worse.
Perhaps in some future time and with some future President, the stars will line up so that White House leadership might be the missing piece to bring us around to efficient and effective approaches to this problem. Even then, don’t hold your breath.
I don't necessarily fault him for this silence. The nation is preoccupied by fairly daunting challenges: two wars, near collapse of the financial system, high unemployment, a dysfunctional Congress, a petro fouling of the Mexican Gulf, 13 million illegal aliens, and continuing threats to national security from terrorist organizations. In addition, the President has to walk the dog and check the kids’ homework. All in a day’s work when you are the leader of the free world. While the toll taken by drug abuse has continued unabated, other problems have taken on greater importance and garner more of the nation’s attention.
However, I think there is something else going on. A couple of decades back, the firm resolve of presidents and PTA officers in the face of the “menace” of drugs was accompanied by great optimism. People believed that drugs could be stopped. With enough grit, energy, and investment, we would have drug-free schools and communities. After all, the U.S. wins wars, and we will win this one as well. Forty years in, people have become cynical and burned out. So many programs have been ineffective, and billions of dollars have been spent, with good intentions, but with no results. Abuse of alcohol, tobacco, and other drugs has waxed and waned, but the trends have been mostly unrelated to what governments and community groups have been doing to bend the consumption curve.
From time to time, people ask me what works in drug abuse prevention. “Works” is a loaded word, because it implies that there is something which might really have a huge impact on adolescent and adult drug abuse. Would that were true. In fact, our only chance of bringing about a less drugged citizenry is a combination of small initiatives, none of which makes much difference by itself, but as a package has some promise. This is not being done in any substantial way, but instead we rely on school-based education, which is mostly ineffective, and we put people in jail, which has mostly made these problems worse.
Perhaps in some future time and with some future President, the stars will line up so that White House leadership might be the missing piece to bring us around to efficient and effective approaches to this problem. Even then, don’t hold your breath.
Monday, July 19, 2010
Raw Milk Rag
Recently I’ve been reading reports about people promoting the virtues of raw (unpasteurized) milk and demanding the right to sell or consume it. As someone who is steeped in conventional public health concepts, I scratch my head and say, “Didn’t we settle that issue 50 years ago?” Apparently not. Within the green movement, which I generally applaud, there is the view that local and small scale is better, and that eating food as close to natural is the ideal. This perspective is reflected in the movie “Avatar” – Western technology is destroying our planet while indigenous simplicity will be our salvation. Coming from a $300 million movie, the premise is simple minded and manipulative, but it resonates with the raw milkers. This is as idiotic as the birthers, who want to contest Obama’s citizenship.
The first recent time I saw this issue discussed was in Michael Feldman’s essay in the NY Times. He was discussing political agitation against Wisconsin state bans on selling raw milk, and coined the phrase “teat party,” because the advocates are chafing against state and federal raw milk rules which impinge on local prerogatives. The question is “Why not let people decide for themselves, rather than government bureaucrats dictating?” This is part of what TEA Partiers mean when they say “Let’s take our government back.” The response is that adults have a right to choose, but the heaviest consumers of milk are children, and they cannot make an informed choice, and therefore should be protected by the state. Note that children are also more vulnerable because their immune systems are less able to fight microbes carried in contaminated milk.
Some people believe that pasteurized milk loses nutritional value, and that the pasteurization process makes milk a kind of “Frankenfood” in the same category as foods irradiated for the same purpose – to stop food borne infectious disease. About half the states prohibit raw milk sale, and the federal government prohibits transport of raw milk across state lines, except for the purpose of pasteurizing the milk in another state or shipping it to a cheese production site. Because of this, raw milk production and sale can only be a small scale operation. It has a smaller environmental impact, and of course, uses less electrical power when the heating process of pasteurization is eliminated.
In our history, milk has been one of the most common sources of food carried illness. We get milk from cows, goats, sheep, and various other mammalian animals. Those animals also have bowel functions, and they are not “barn broken.” We don’t control when and where they drop manure. It might be theoretically possible to assure no exposure of milk with manure, but this would require a small ratio of animals per dairy worker and intense use of technology. This would not be economically viable for most diary farms. It is unlikely that farmers can sustain production conditions to prevent the deaths and serious illnesses we have seen linked to raw milk.
There is also the claim that raw milk has protective factors against a number of illnesses, such as allergies. Not true, or at least no evidence.
In addition, raw milk advocates say it tastes better. This is a subjective point, that is not right or wrong, but taste differences may have more to do with homogenization, which is also usually not done with raw milk.
So here is the stalemate with our values. We value independence and personal liberties, and this is a precious quality of our life in the U.S. At the same time we value life and health promotion. Everyone in a sense is “prolife,” in spite of our differences over abortion or end of life decision-making. The libertarian view seems to be gaining strength in 2010. I just wish it was guided by facts, not just whimsy.
The first recent time I saw this issue discussed was in Michael Feldman’s essay in the NY Times. He was discussing political agitation against Wisconsin state bans on selling raw milk, and coined the phrase “teat party,” because the advocates are chafing against state and federal raw milk rules which impinge on local prerogatives. The question is “Why not let people decide for themselves, rather than government bureaucrats dictating?” This is part of what TEA Partiers mean when they say “Let’s take our government back.” The response is that adults have a right to choose, but the heaviest consumers of milk are children, and they cannot make an informed choice, and therefore should be protected by the state. Note that children are also more vulnerable because their immune systems are less able to fight microbes carried in contaminated milk.
Some people believe that pasteurized milk loses nutritional value, and that the pasteurization process makes milk a kind of “Frankenfood” in the same category as foods irradiated for the same purpose – to stop food borne infectious disease. About half the states prohibit raw milk sale, and the federal government prohibits transport of raw milk across state lines, except for the purpose of pasteurizing the milk in another state or shipping it to a cheese production site. Because of this, raw milk production and sale can only be a small scale operation. It has a smaller environmental impact, and of course, uses less electrical power when the heating process of pasteurization is eliminated.
In our history, milk has been one of the most common sources of food carried illness. We get milk from cows, goats, sheep, and various other mammalian animals. Those animals also have bowel functions, and they are not “barn broken.” We don’t control when and where they drop manure. It might be theoretically possible to assure no exposure of milk with manure, but this would require a small ratio of animals per dairy worker and intense use of technology. This would not be economically viable for most diary farms. It is unlikely that farmers can sustain production conditions to prevent the deaths and serious illnesses we have seen linked to raw milk.
There is also the claim that raw milk has protective factors against a number of illnesses, such as allergies. Not true, or at least no evidence.
In addition, raw milk advocates say it tastes better. This is a subjective point, that is not right or wrong, but taste differences may have more to do with homogenization, which is also usually not done with raw milk.
So here is the stalemate with our values. We value independence and personal liberties, and this is a precious quality of our life in the U.S. At the same time we value life and health promotion. Everyone in a sense is “prolife,” in spite of our differences over abortion or end of life decision-making. The libertarian view seems to be gaining strength in 2010. I just wish it was guided by facts, not just whimsy.
Sunday, July 18, 2010
Health Care Reform Triangulation
Today on the front page of the NY Times was a feature article about an effort by health insurance companies to offer more restricted plans for less money. As consumers we are silent bystanders to these negotiations, since the insurers deal mostly with employers. Companies large and small are struggling with the cost of providing health insurance for their workers. These newer insurance products present lower costs, or at least lower increases in cost in exchange for offering companies (and workers) fewer choices.
One of the selling points repeated loudly and often by the President was that with the health care reform package no one would lose their insurance; they could keep the coverage they had or opt into something better. The President was right to a degree. The government won't force these decisions, but the health care market is spiraling out of control; this would have been true even if Obama had never uttered the words "health care reform." Our current system is unsustainable. No segment of society, not government, not corporations, not individuals (except the very wealthy) will be able to afford our health care system going forward. This is not even addressing the serious failures of our system in protecting and promoting health. We have a lousy system now, but we can't afford it much longer. Though much maligned by Obama’s opponents, the European systems are wildly popular with their citizens, less costly, and get better results.
As the Times article illustrates, many people may lose their current health insurance plans, not because of health care reform, but because employers can no longer afford plans we've taken for granted in the past. This would be true even if Obama had never come on the scene.
The focal point of what we value can be visualized by a triangle, with cost, access, and choice at the points. Up until now, choice has been in the ascendancy. Americans want to choose their doctors, their drugs, their hospital. Of course most consumers' choices in this regard are not guided by evidence of value. Data to guide these choices has not been available, and so we are persuaded by marketing ploys and superficial indicators. This is beginning to change, but slowly.
The primary driver of this year's health care reform legislation has been to increase access, bringing in the 40 million Americans with no health insurance, and therefore no choice except emergency room medicine. While universal access is a worthy goal, and something demanded by social justice, it will increase cost unless adjustments are made elsewhere in the system. If we want to increase access without increasing cost, we have to limit choice.
Some of the most vocal opponents of the health care reform proposals which passed this year claim that we will have to ration care. What they really mean is "I have good care now, and don't want to sacrifice so that those shut out of the system can be served." Of course we ration now, but those excluded, by and large, have no voice in the political system. In order to hold down cost while maintaining choice, we limit access.
Researchers at Dartmouth Medical School have clearly shown that unlimited access is not really a good thing. Not only does it drive up cost, it also drives up waste. Those researchers (Google Dartmouth Atlas) estimate that somewhere in the neighborhood of $700 billion per year is wasted. This expense might enrich providers, but does nothing for individual or public health. This represents a fourth to a third of the nation's health care expense. Costs come from duplication of services, or providing services which do not benefit patients. In other words, we are victims of inefficiency and gaming the system, charging for things that shouldn't be provided in the first place. This latter practice is so common it is a standard of care in some places. It is theft in plain sight.
It is clear that there is much to be done to reach the potential we have as a nation, finding a better balance between the best of open markets and private enterprise and being sure that health protection and promotion is the goal, not just a business plan.
One of the selling points repeated loudly and often by the President was that with the health care reform package no one would lose their insurance; they could keep the coverage they had or opt into something better. The President was right to a degree. The government won't force these decisions, but the health care market is spiraling out of control; this would have been true even if Obama had never uttered the words "health care reform." Our current system is unsustainable. No segment of society, not government, not corporations, not individuals (except the very wealthy) will be able to afford our health care system going forward. This is not even addressing the serious failures of our system in protecting and promoting health. We have a lousy system now, but we can't afford it much longer. Though much maligned by Obama’s opponents, the European systems are wildly popular with their citizens, less costly, and get better results.
As the Times article illustrates, many people may lose their current health insurance plans, not because of health care reform, but because employers can no longer afford plans we've taken for granted in the past. This would be true even if Obama had never come on the scene.
The focal point of what we value can be visualized by a triangle, with cost, access, and choice at the points. Up until now, choice has been in the ascendancy. Americans want to choose their doctors, their drugs, their hospital. Of course most consumers' choices in this regard are not guided by evidence of value. Data to guide these choices has not been available, and so we are persuaded by marketing ploys and superficial indicators. This is beginning to change, but slowly.
The primary driver of this year's health care reform legislation has been to increase access, bringing in the 40 million Americans with no health insurance, and therefore no choice except emergency room medicine. While universal access is a worthy goal, and something demanded by social justice, it will increase cost unless adjustments are made elsewhere in the system. If we want to increase access without increasing cost, we have to limit choice.
Some of the most vocal opponents of the health care reform proposals which passed this year claim that we will have to ration care. What they really mean is "I have good care now, and don't want to sacrifice so that those shut out of the system can be served." Of course we ration now, but those excluded, by and large, have no voice in the political system. In order to hold down cost while maintaining choice, we limit access.
Researchers at Dartmouth Medical School have clearly shown that unlimited access is not really a good thing. Not only does it drive up cost, it also drives up waste. Those researchers (Google Dartmouth Atlas) estimate that somewhere in the neighborhood of $700 billion per year is wasted. This expense might enrich providers, but does nothing for individual or public health. This represents a fourth to a third of the nation's health care expense. Costs come from duplication of services, or providing services which do not benefit patients. In other words, we are victims of inefficiency and gaming the system, charging for things that shouldn't be provided in the first place. This latter practice is so common it is a standard of care in some places. It is theft in plain sight.
It is clear that there is much to be done to reach the potential we have as a nation, finding a better balance between the best of open markets and private enterprise and being sure that health protection and promotion is the goal, not just a business plan.
Saturday, July 17, 2010
Vaccine Vicissitudes
Most often vaccination technology is traced back to 1796 when Edward Jenner had success in England protecting people against smallpox. However, it wasn't until the 20th century that vaccines really made an impact on the public's health. Beginning early in the century, and accelerating after WWII, the great microbial scourges were de-clawed in a stunning triumph of scientific ingenuity. The incidence of smallpox, polio, measles, diphtheria, whooping cough, mumps, and rubella all declined by about 100% in the 100 years ending in 2000. This was important in the dramatic increase of U.S. life expectancy from about 42 years in 1900 to about 78 today. People survived these threats to children and lived to almost complete their genetic potential for life expectancy. Ironically, this allowed our bodies to live long enough to develop chronic diseases of aging. Nevertheless, no one should pine for the bad old days when at least one in ten infants, and many older children perished, mostly from infections.
In recent years there has been a persistent myth in the popular media that vaccines are the cause of autism. Let's be clear: no valid science exists to link vaccination with autism. This is another case where people have trouble with uncertainty, but look for something to blame when unknown is less satisfying.
Some of the interesting new vaccination innovations include the HPV vaccine, which protects young people against papilloma virus infections, and subsequently, protects women against cervical cancer. This is a fairly new vaccine, and some people feel there was too much hurry bringing the vaccine to market. There is no evidence of danger, but the effectiveness may be less than was hoped. Another new vaccine is one for shingles, and recommended for people over the age of 60, when shingles becomes quite common. Because shingles is rarely life threatening, or even severe enough to require hospitalization, some insurance companies are limiting coverage. Their attitude is "Quit being such a wimp about it. You'll get over it and be just fine." Perhaps as the vaccine grows in popularity the price will drop.
There is research being done on a vaccine to prevent smoking initiation and discourage continued smoking. The mechanism is to modify the nicotine molecule so that it is not able to enter the brain and stimulate the receptors which make the drug so reinforcing. In this case, smoking would not provide any benefit, leading youth not to go beyond experimenting and confirmed smokers to extinguish their habits. Stay tuned. Were this technology ever to reach the market, it would be great news for millions of smokers. There is parallel research going on to harness vaccine manipulation of the endocrine system, making food less reinforcing. At this point, there is only preliminary evidence that such an approach could actually work; it is probably many years away in any case.
The two elephants in the room for traditional vaccine applications are HIV/AIDS and malaria. These two diseases result in about 2 million and 850,000 deaths each year on planet earth. We don't have exact statistics because the regions of the world where they wreak the most havoc, such as sub-Saharan Africa, have inadequate systems to monitor incidence and causes of death. The good news is that there is research to develop vaccines for each of these infections, and there is some optimism that in the not too distant future there will be success. In terms of public health impact, a Nobel Prize will be in order.
Unfortunately, in spite of the tragic toll taken by HIV and malaria, any vaccines would be considered "orphan drugs." The lion's share of pharmaceutical research is done in the private sector, and this is one of the most profitable enterprises. This industry without doubt is responsible for true "wonder" drugs which have improved the lives of millions of patients. However, a market-driven drug industry means there is a whole category of drugs, so called "orphans" which because their market potential is limited, are never brought to market. For this reason there are illness for which we have drug solutions, but because they are rare, there is no business incentive to make the investments needed to bring them to market. HIV and malaria are in this category. The largest market for any vaccines would be in places where most of the patients live-places where people can't pay, and even if they could, it is a one time payment. Companies are most interested in drugs which people take on a daily basis for years at a time. Vaccines are usually not like that. It is likely that HIV and malaria vaccine research will have to be largely subsidized by governments and humanitarian organizations, and their distribution will not be sponsored by corporations.
Life without vaccines would be unfathomable. There is reason to expect that they will make life even better, promoting health for all in the future.
In recent years there has been a persistent myth in the popular media that vaccines are the cause of autism. Let's be clear: no valid science exists to link vaccination with autism. This is another case where people have trouble with uncertainty, but look for something to blame when unknown is less satisfying.
Some of the interesting new vaccination innovations include the HPV vaccine, which protects young people against papilloma virus infections, and subsequently, protects women against cervical cancer. This is a fairly new vaccine, and some people feel there was too much hurry bringing the vaccine to market. There is no evidence of danger, but the effectiveness may be less than was hoped. Another new vaccine is one for shingles, and recommended for people over the age of 60, when shingles becomes quite common. Because shingles is rarely life threatening, or even severe enough to require hospitalization, some insurance companies are limiting coverage. Their attitude is "Quit being such a wimp about it. You'll get over it and be just fine." Perhaps as the vaccine grows in popularity the price will drop.
There is research being done on a vaccine to prevent smoking initiation and discourage continued smoking. The mechanism is to modify the nicotine molecule so that it is not able to enter the brain and stimulate the receptors which make the drug so reinforcing. In this case, smoking would not provide any benefit, leading youth not to go beyond experimenting and confirmed smokers to extinguish their habits. Stay tuned. Were this technology ever to reach the market, it would be great news for millions of smokers. There is parallel research going on to harness vaccine manipulation of the endocrine system, making food less reinforcing. At this point, there is only preliminary evidence that such an approach could actually work; it is probably many years away in any case.
The two elephants in the room for traditional vaccine applications are HIV/AIDS and malaria. These two diseases result in about 2 million and 850,000 deaths each year on planet earth. We don't have exact statistics because the regions of the world where they wreak the most havoc, such as sub-Saharan Africa, have inadequate systems to monitor incidence and causes of death. The good news is that there is research to develop vaccines for each of these infections, and there is some optimism that in the not too distant future there will be success. In terms of public health impact, a Nobel Prize will be in order.
Unfortunately, in spite of the tragic toll taken by HIV and malaria, any vaccines would be considered "orphan drugs." The lion's share of pharmaceutical research is done in the private sector, and this is one of the most profitable enterprises. This industry without doubt is responsible for true "wonder" drugs which have improved the lives of millions of patients. However, a market-driven drug industry means there is a whole category of drugs, so called "orphans" which because their market potential is limited, are never brought to market. For this reason there are illness for which we have drug solutions, but because they are rare, there is no business incentive to make the investments needed to bring them to market. HIV and malaria are in this category. The largest market for any vaccines would be in places where most of the patients live-places where people can't pay, and even if they could, it is a one time payment. Companies are most interested in drugs which people take on a daily basis for years at a time. Vaccines are usually not like that. It is likely that HIV and malaria vaccine research will have to be largely subsidized by governments and humanitarian organizations, and their distribution will not be sponsored by corporations.
Life without vaccines would be unfathomable. There is reason to expect that they will make life even better, promoting health for all in the future.
Friday, July 16, 2010
Health Inequality, continued
One of our national health goals, as articulated by the Healthy People project, is to decrease health disparities, to make it possible for all groups to enjoy the rates of health and freedom from disease enjoyed by those groups with the best health. This is a tall order, and won't be achieved any time soon, but in recent years we have finally come to grips with the social justice dimensions of health status.
So here is a case study. Since the early to mid 1960s, the nation has been conducting an anti-tobacco campaign. Of course that campaign has been blocked by Big Tobacco, farmers in traditional tobacco states, cigarette retailers, and the hospitality industry. Nevertheless, there has been a continuous parade of small health promotion victories as we have learned more effective ways to discourage smoking by youth, developed better smoking cessation techniques, and put in place more public policies to block the promotion of tobacco products and reduce the presence of public smoking in workplaces and communities.
While these victories can and should be celebrated, we still have 45 million smokers in the U.S. The smoker proportion of the population has dramatically shrunk, from about 55% of adult men to now around 22%, and the absolute number of smokers is smaller than in years past, but 45 million still presents a huge challenge to the public's health. It represents an unacceptable drain on our health care system. What has happened over the years is that the profile of smokers has changed. Whereas in the past, smoking was more evenly distributed among all segments, predominantly males, but now it is increasingly clustered among low income groups with minimal education. Twenty years ago, the stereotype smoker was a white, middle class sales representative. Now, the typical smoker is a low income minority person in a blue collar job.
The reasons for this shift are many. Poorly educated persons are less likely to be aware of the overwhelming case against smoking and the benefits of quitting. People on the lower rungs of socioeconomic status often have less of a future orientation, and tend to feel powerless, even when it comes to managing their own health. They are less connected to national media, in which the dangers of smoking are widely accepted with no reservations. Because they are less likely to be getting regular health care, and in the setting where they get health care (e.g. an emergency room) they are unlikely to form a long term therapeutic relationship with the same provider, and therefore are less likely to have a physician who is mentoring them over time to quit. In addition, low income minority neighborhoods and groups are special targets of tobacco marketing. There are even brands of cigarettes designed to appeal to those segments of the market. Finally, to the extent that cessation can be aided by access to resources like Chantix, these groups have a more difficult time quitting.
The above description should illustrate that solving health inequities is more than giving people access to medical services and telling them health information. It requires a comprehensive approach that reaches even into the basic structures of society. Jesse Jackson is quoted with saying (I'm paraphrasing) "Rather than promoting school choice, how about working for a society in which every school is choice and every child is chosen." That is not our world, and until it is, health inequity will continue to diminish the potential of our nation.
So here is a case study. Since the early to mid 1960s, the nation has been conducting an anti-tobacco campaign. Of course that campaign has been blocked by Big Tobacco, farmers in traditional tobacco states, cigarette retailers, and the hospitality industry. Nevertheless, there has been a continuous parade of small health promotion victories as we have learned more effective ways to discourage smoking by youth, developed better smoking cessation techniques, and put in place more public policies to block the promotion of tobacco products and reduce the presence of public smoking in workplaces and communities.
While these victories can and should be celebrated, we still have 45 million smokers in the U.S. The smoker proportion of the population has dramatically shrunk, from about 55% of adult men to now around 22%, and the absolute number of smokers is smaller than in years past, but 45 million still presents a huge challenge to the public's health. It represents an unacceptable drain on our health care system. What has happened over the years is that the profile of smokers has changed. Whereas in the past, smoking was more evenly distributed among all segments, predominantly males, but now it is increasingly clustered among low income groups with minimal education. Twenty years ago, the stereotype smoker was a white, middle class sales representative. Now, the typical smoker is a low income minority person in a blue collar job.
The reasons for this shift are many. Poorly educated persons are less likely to be aware of the overwhelming case against smoking and the benefits of quitting. People on the lower rungs of socioeconomic status often have less of a future orientation, and tend to feel powerless, even when it comes to managing their own health. They are less connected to national media, in which the dangers of smoking are widely accepted with no reservations. Because they are less likely to be getting regular health care, and in the setting where they get health care (e.g. an emergency room) they are unlikely to form a long term therapeutic relationship with the same provider, and therefore are less likely to have a physician who is mentoring them over time to quit. In addition, low income minority neighborhoods and groups are special targets of tobacco marketing. There are even brands of cigarettes designed to appeal to those segments of the market. Finally, to the extent that cessation can be aided by access to resources like Chantix, these groups have a more difficult time quitting.
The above description should illustrate that solving health inequities is more than giving people access to medical services and telling them health information. It requires a comprehensive approach that reaches even into the basic structures of society. Jesse Jackson is quoted with saying (I'm paraphrasing) "Rather than promoting school choice, how about working for a society in which every school is choice and every child is chosen." That is not our world, and until it is, health inequity will continue to diminish the potential of our nation.
Tuesday, July 13, 2010
Health Inequality
Some aspects of your health are determined at conception, including most significantly, how long you can expect to live. Other influences occur during your mother's pregnancy, such as having enough oxygen coming into your developing body and not being exposed to alcohol or other drugs. We are very vulnerable during the first year; compared to children ages 5-14, infants have a death rate 40 times greater. Most of us do survive that first year, though the odds are much scarier in poor nations such as Afghanistan, where infants die at a rate 25 times greater than in the U.S.
From childhood through adolescence and into adulthood, we are impacted by our lifestyles (e.g. smoking, exercise, safety habits), by our access to medical and other human services, and our physical and social surroundings. Social surroundings can be very supportive. For example, if people belong to a church, synagogue, mosque or temple, and participate in a congregation, their health will usually be better than those not so connected. On the other hand, many people are lacking in community and social support, and this results in selectively higher rates of death and disease.
Consider this slide: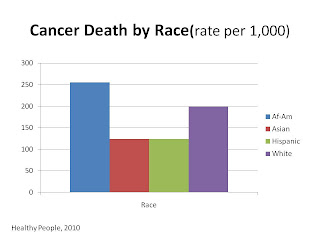 It shows U.S. cancer deaths by racial group. Asians and Hispanics have lower cancer deaths while whites are in a middle range, with African Americans having the highest rates. The question is, why is there such a huge gap between groups, and why don't all groups have the lowest rates? Though it is impossible to make the cancer death rate be zero, we ought to be able to achieve the same low rate for all. Unfortunately, almost no progress has been made to make health equal for all. Even in cases where death rates have come down for all, the mortality gap between the highest and lowest has not narrowed. So what causes health inequality?
It shows U.S. cancer deaths by racial group. Asians and Hispanics have lower cancer deaths while whites are in a middle range, with African Americans having the highest rates. The question is, why is there such a huge gap between groups, and why don't all groups have the lowest rates? Though it is impossible to make the cancer death rate be zero, we ought to be able to achieve the same low rate for all. Unfortunately, almost no progress has been made to make health equal for all. Even in cases where death rates have come down for all, the mortality gap between the highest and lowest has not narrowed. So what causes health inequality?
To be continued....
From childhood through adolescence and into adulthood, we are impacted by our lifestyles (e.g. smoking, exercise, safety habits), by our access to medical and other human services, and our physical and social surroundings. Social surroundings can be very supportive. For example, if people belong to a church, synagogue, mosque or temple, and participate in a congregation, their health will usually be better than those not so connected. On the other hand, many people are lacking in community and social support, and this results in selectively higher rates of death and disease.
Consider this slide:

To be continued....
Monday, July 12, 2010
Values conflict and health promotion
Victor Hugo is quoted as saying "All the forces in the world are not so powerful as an idea whose time has come." It’s an inspiring vision for those wanting to change the world. Once in a great while it may prove to be true, but more often it is more realistic to see an ecology of ideas, in which perspectives around an idea are checking and balancing one another, trying to obtain critical mass of support to carry the day. This blog is not about politics, but health policy is part of the idea ecology, and often health promotion strategies do battle with competing perspectives in the political arena. Public health and other health professionals are guided by ethical standards, so often are at a disadvantage against political adversaries, who are less concerned about truth or accuracy.
Usually health promotion advice is tame and not controversial. People will act on it, or not, but usually don't get angry when they hear it. Americans love high fat foods, and consume far too much fat, salt, and sugar. This is widely known, but gets almost no active opposition, other than the food producers continuing to sell us unhealthy foods, and we continue to buy them. No important groups or individuals are trying to tell us that fat, salt and sugar are good for us, or condemning the health care system for trying to help us cut back on those unhealthy foods.
On the other hand, health promotion often relies on policy to bring about health improvement. For example, we have state laws requiring people to wear seat belts while they are in a moving vehicle. That's a policy solution to a problem that could be served by a public education campaign alone. We could just encourage and try to persuade people to wear seat belts, but instead we also have seat belt laws. The rationale is that education alone wasn't getting the job done (back in the 70s and 80s) so that large numbers of people still didn't buckle up. The number of highway deaths was so great that government (that's us) decided the education campaigns needed to be reinforced with a legal policy. Policy and education, together, have been successful, as the rate of highway fatalities has dropped dramatically compared to what it was in the 50s, 60s and 70s. However, many people rankle against health promotion policies, when they think their rights and freedoms are trampled.
In my state there is a U.S. Senate candidate who is a physician in his day job. He is opposed to smoking ordinances, where smoking is legally prohibited in workplaces and anywhere the public is served, such as restaurants. These ordinances are a policy solution. We could rely on public education encouraging smoking cessation, and we could encourage businesses to voluntarily ban smoking in their own establishments. More and more communities are enacting this policy to protect nonsmokers, including people exposed while they do their jobs. It is considered necessary because there are thousands of deaths associated with second hand smoke, and other options, such as no smoking sections don’t work.
This candidate opposes smoking ordinances, not because he thinks smoking-related illnesses are a good thing or because he has a financial interest in the tobacco industry, but because he values private property rights over health concerns. It is a values question.
How high on the scale of things do we place health? Do we think it is important to protect all people from exposure to tobacco smoke, or do we consider individual choice and property rights to take precedence? Do we think it more important to protect the health of Gulf of Mexico water and shore land, or is it more important to protect economic interests and drill baby, drill. Should we aggressively expect food producers to make and sell healthier foods, or should we instead try to change consumer demand by public education, relying on the market to eventually come around to healthier products? Do we demand unlimited access to guns as a right, or do we take steps to limit the homicides and suicides linked to the large number of firearms in our society?
It is hard to determine the political will these days. Some individuals and groups put a premium on individual liberty and level "a pox on your house" to those who believe that government policies are important to bring about a community where most people can thrive. Does that perspective really represent most people, or just a vocal minority? Maximum individual liberty at the cost of poor health doesn't seem like a way to assure that all can pursuit happiness.
Usually health promotion advice is tame and not controversial. People will act on it, or not, but usually don't get angry when they hear it. Americans love high fat foods, and consume far too much fat, salt, and sugar. This is widely known, but gets almost no active opposition, other than the food producers continuing to sell us unhealthy foods, and we continue to buy them. No important groups or individuals are trying to tell us that fat, salt and sugar are good for us, or condemning the health care system for trying to help us cut back on those unhealthy foods.
On the other hand, health promotion often relies on policy to bring about health improvement. For example, we have state laws requiring people to wear seat belts while they are in a moving vehicle. That's a policy solution to a problem that could be served by a public education campaign alone. We could just encourage and try to persuade people to wear seat belts, but instead we also have seat belt laws. The rationale is that education alone wasn't getting the job done (back in the 70s and 80s) so that large numbers of people still didn't buckle up. The number of highway deaths was so great that government (that's us) decided the education campaigns needed to be reinforced with a legal policy. Policy and education, together, have been successful, as the rate of highway fatalities has dropped dramatically compared to what it was in the 50s, 60s and 70s. However, many people rankle against health promotion policies, when they think their rights and freedoms are trampled.
In my state there is a U.S. Senate candidate who is a physician in his day job. He is opposed to smoking ordinances, where smoking is legally prohibited in workplaces and anywhere the public is served, such as restaurants. These ordinances are a policy solution. We could rely on public education encouraging smoking cessation, and we could encourage businesses to voluntarily ban smoking in their own establishments. More and more communities are enacting this policy to protect nonsmokers, including people exposed while they do their jobs. It is considered necessary because there are thousands of deaths associated with second hand smoke, and other options, such as no smoking sections don’t work.
This candidate opposes smoking ordinances, not because he thinks smoking-related illnesses are a good thing or because he has a financial interest in the tobacco industry, but because he values private property rights over health concerns. It is a values question.
How high on the scale of things do we place health? Do we think it is important to protect all people from exposure to tobacco smoke, or do we consider individual choice and property rights to take precedence? Do we think it more important to protect the health of Gulf of Mexico water and shore land, or is it more important to protect economic interests and drill baby, drill. Should we aggressively expect food producers to make and sell healthier foods, or should we instead try to change consumer demand by public education, relying on the market to eventually come around to healthier products? Do we demand unlimited access to guns as a right, or do we take steps to limit the homicides and suicides linked to the large number of firearms in our society?
It is hard to determine the political will these days. Some individuals and groups put a premium on individual liberty and level "a pox on your house" to those who believe that government policies are important to bring about a community where most people can thrive. Does that perspective really represent most people, or just a vocal minority? Maximum individual liberty at the cost of poor health doesn't seem like a way to assure that all can pursuit happiness.
Sunday, July 11, 2010
Donald Berwick, Health Care Reform, and Health Promotion
This week President Obama appointed Donald Berwick to be director of Centers for Medicare and Medicaid Services. This is the federal government unit charged with managing the Medicare program and the federal portion of the Medicaid program. Because those two programs capture such a large segment of the health care enterprise, they have a huge impact on the system as a whole, including private providers and hospitals. This appointment has been loudly criticized, mostly but not exclusively by those opposed to Obama's agenda. The appointment was made during a Congressional recess, and thereby avoided Senate approval, which was unlikely because conservatives would have filibustered and killed the nomination. This is a sad commentary on the current state of our political system, which seems to be only about winning elections rather than making the country better through effective use of government processes and structures. I digress.
Our current health system is broken and fiscally unsustainable. In spite of spending substantially more per person than any other nation, we rank relatively low in outcomes among the modern, developed countries. This is a national disgrace. In the 1980s there was a national scandal surrounding military purchasing and the expenditures of the Department of Defense. The $600 hammer became notorious as emblematic of the abuses in the system. There is a very similar pattern which happens every day in the health care system. Costs are incurred and paid by either government or the private sector, which are either unjustifiable high, disconnected from any objective standard of value, and many times even unnecessary at all. The Tea Party advocates are loud opponents of what they consider excessive and unnecessary taxes, but don't seem to mind being scammed by market-driven health care.
Into the picture comes Donald Berwick. His claim to fame can be summarized by "increasing quality of care." How boring, yet if the ideas he promotes were implemented, we could save thousands of deaths and hospital days each year, save hundreds of millions of dollars of health care expense, and efficiently cover all Americans with basic health care without increasing budget deficits and the national debt. I hope he is successful in bringing about change to the extent permitted by the limits of the CMMS position.
Overlayed on this can be thoughts about prevention. The old adage is "an ounce of prevention is worth a pound of cure." Partly true, partly not. The health care proposals passed this year include provisions for preventive care and health promotion. Some of those ideas will save money, but many of them will improve health without necessarily saving money. Here is the reason. In a humane society, we should use all the tools we have to prevent people getting influenza. There are about 35,000 flu deaths in a typical year, not counting pandemics like swine flu or bird flu. If every person was immunized, most of those deaths would not occur. However, the cost of universal immunization may be greater than the cost of treating the people who get sick. Prevention of flu may cost more money than it saves, but will improve quantity and quality of life. Various prevention and health promotion practices can be analyzed in this way.
Usually individuals can save money by simple lifestyle measures of eating healthfully, being physically active, getting regular sleep, avoiding tobacco and excess alcohol, safe driving, and so forth. It is more complicated when prevention becomes a society-based effort or a service of the health care system.
The thing that Donald Berwick brings to health care reform is a dogged insistence that what we do is informed and guided by data and evidence - not a knee-jerk response: government bad, unfettered market-driven good.
Our current health system is broken and fiscally unsustainable. In spite of spending substantially more per person than any other nation, we rank relatively low in outcomes among the modern, developed countries. This is a national disgrace. In the 1980s there was a national scandal surrounding military purchasing and the expenditures of the Department of Defense. The $600 hammer became notorious as emblematic of the abuses in the system. There is a very similar pattern which happens every day in the health care system. Costs are incurred and paid by either government or the private sector, which are either unjustifiable high, disconnected from any objective standard of value, and many times even unnecessary at all. The Tea Party advocates are loud opponents of what they consider excessive and unnecessary taxes, but don't seem to mind being scammed by market-driven health care.
Into the picture comes Donald Berwick. His claim to fame can be summarized by "increasing quality of care." How boring, yet if the ideas he promotes were implemented, we could save thousands of deaths and hospital days each year, save hundreds of millions of dollars of health care expense, and efficiently cover all Americans with basic health care without increasing budget deficits and the national debt. I hope he is successful in bringing about change to the extent permitted by the limits of the CMMS position.
Overlayed on this can be thoughts about prevention. The old adage is "an ounce of prevention is worth a pound of cure." Partly true, partly not. The health care proposals passed this year include provisions for preventive care and health promotion. Some of those ideas will save money, but many of them will improve health without necessarily saving money. Here is the reason. In a humane society, we should use all the tools we have to prevent people getting influenza. There are about 35,000 flu deaths in a typical year, not counting pandemics like swine flu or bird flu. If every person was immunized, most of those deaths would not occur. However, the cost of universal immunization may be greater than the cost of treating the people who get sick. Prevention of flu may cost more money than it saves, but will improve quantity and quality of life. Various prevention and health promotion practices can be analyzed in this way.
Usually individuals can save money by simple lifestyle measures of eating healthfully, being physically active, getting regular sleep, avoiding tobacco and excess alcohol, safe driving, and so forth. It is more complicated when prevention becomes a society-based effort or a service of the health care system.
The thing that Donald Berwick brings to health care reform is a dogged insistence that what we do is informed and guided by data and evidence - not a knee-jerk response: government bad, unfettered market-driven good.
Saturday, July 10, 2010
Is it pointless?
My mother has had a subscription to Prevention magazine for probably 20 years; it still arrives in the mail each month. Not only did she read the magazine, but read many books and articles published in other places regarding how to have the best health. Aside from reading a lot about health, she was quite conscientious about practicing what she was reading, at least as far as diet. She was quite disciplined about maintaining a healthy lifestyle, with perhaps the exception of exercise which she did not do on a routine basis.
She is now in her late 80s, living in a nursing home. She is confined to bed unless someone gets her out of it into a wheel chair, and her life is confined to one room most of the time. She is awake and can interact with people. She knows what is going on around her, and still knows everyone she might be expected to know. On the other hand, her thoughts are often scrambled, lacking recognition about what is real and what isn't. Sometimes conversing with her is like talking to a schizophrenic person because she believes and tells things which are clearly impossible, yet has certainty that they are true.
So was all of her effort to live a healthy lifestyle a waste of time? Was it all a delusion to think by conscientious effort she could live life more abundantly? For anyone, is there a point to practicing health promotion principles?
When I was young and inexperienced my answer would have been a rousing YES! When it comes to health, "I am the master of my fate, I am the captain of my soul," to quote Invictus. Now, my answer is a guarded yes. Because of the intricacies of body parts and functions, down to the cellular and molecular level, and the great range of forces on the outside which influence our health, it is not possible to think about health as a simple transaction: "If you do these five things, you will live in good health for a long and prosperous life." The truth is health promotion is one part discipline and one part crap shoot.
We try to discover things which statistically increase the odds of living well. What is statistically probable for a population or group does not always play out for every individual. This explains why there are a few nonsmokers who get lung cancer while a few smokers don't. Statistically, the odds are much better that if you don't smoke, your health will be much better. About some things we are much more sure, and the evidence is very convincing. Other things will have evidence only suggestive, but not certain.
I choose to follow those things which are most promising. I may win or lose, but will take the odds every time.
By the way, my mother has passed the average life expectancy for women her age by about eight years - a partial victory.
She is now in her late 80s, living in a nursing home. She is confined to bed unless someone gets her out of it into a wheel chair, and her life is confined to one room most of the time. She is awake and can interact with people. She knows what is going on around her, and still knows everyone she might be expected to know. On the other hand, her thoughts are often scrambled, lacking recognition about what is real and what isn't. Sometimes conversing with her is like talking to a schizophrenic person because she believes and tells things which are clearly impossible, yet has certainty that they are true.
So was all of her effort to live a healthy lifestyle a waste of time? Was it all a delusion to think by conscientious effort she could live life more abundantly? For anyone, is there a point to practicing health promotion principles?
When I was young and inexperienced my answer would have been a rousing YES! When it comes to health, "I am the master of my fate, I am the captain of my soul," to quote Invictus. Now, my answer is a guarded yes. Because of the intricacies of body parts and functions, down to the cellular and molecular level, and the great range of forces on the outside which influence our health, it is not possible to think about health as a simple transaction: "If you do these five things, you will live in good health for a long and prosperous life." The truth is health promotion is one part discipline and one part crap shoot.
We try to discover things which statistically increase the odds of living well. What is statistically probable for a population or group does not always play out for every individual. This explains why there are a few nonsmokers who get lung cancer while a few smokers don't. Statistically, the odds are much better that if you don't smoke, your health will be much better. About some things we are much more sure, and the evidence is very convincing. Other things will have evidence only suggestive, but not certain.
I choose to follow those things which are most promising. I may win or lose, but will take the odds every time.
By the way, my mother has passed the average life expectancy for women her age by about eight years - a partial victory.
Friday, July 9, 2010
Health and the Unknown
I'm always surprised when I see otherwise intelligent people banking on diets, treatments, or "medical" devices which have no basis in science, and no more evidence than testimonials and promises. It is certainly true that some people have had opportunities to learn about medical and health science, and so are better informed. Those not so fortunate are like most of us regarding cars. It used to be possible for the average person to fix many things that went wrong with a car; that option is shrinking as cars have become more and more technology driven, with complex circuits and computer components. As medical science has advanced at a stunning rate over the last 100 years, our bodies don't break down as often, somewhat like our experience with cars. It is also harder and harder for the average person to keep up with all this new health knowledge.
On the other hand there is still much unknown about health and medical science, even by the experts. Why do some people get cancer, while similar people don't? Why do some people survive cancer while others don't? Why is weight management easy for some people and almost impossible for others. There are no answers for these and many more questions.
Into that void, our minds want to place something. We have to attribute causes to things. It is too unsettling to admit that we don't have control over everything. This presents a business opportunity to entrepreneurs, some sincere, others cynical. They take advantage of our grasping for answers when none exist.
Far better to apply evidence-based health promotion or treatment practices when we can, but otherwise to enjoy our days as they come.
On the other hand there is still much unknown about health and medical science, even by the experts. Why do some people get cancer, while similar people don't? Why do some people survive cancer while others don't? Why is weight management easy for some people and almost impossible for others. There are no answers for these and many more questions.
Into that void, our minds want to place something. We have to attribute causes to things. It is too unsettling to admit that we don't have control over everything. This presents a business opportunity to entrepreneurs, some sincere, others cynical. They take advantage of our grasping for answers when none exist.
Far better to apply evidence-based health promotion or treatment practices when we can, but otherwise to enjoy our days as they come.
Thursday, July 8, 2010
Survival of the Fittest, part 4
Natural selection also has a social dimension which has a profound, and mostly unrecognized impact on health status. In a sense, it isn't really "natural" selection because the factors are socially determined, and not distributed by merit. Whether it is in career ladders, little league soccer, reality TV, small business survival, college admissions, and even dating, it is understood that personal qualities, effort and social standing create a pecking order of big winners, smaller winners, smaller losers, and bigger losers. People will compete and the "fittest" will have the most success (i.e. will survive).
Over the last 25 years what is known as the "social gradient" has been described by careful population research. This means that your position on the socioeconomic scale or social hierarchy will have a profound effect on your health. This is true even if we control for lifestyle(e.g smoking, obesity) and access to health care. People at the highest level of education, income, and social standing have the highest degree of health status. Those a notch lower have a little bit poorer health status, and so on down to the lowest levels of society, in which people have by far the poorest health status.
It can be argued that social determination of your health is inherently unfair. However, most people are apathetic because it seems so hopeless, as a practical matter to contemplate eliminating poverty or substandard housing. We know how to do these things in principle, but have had little success with real people in real communities.
This is certainly in the mainstream of progressive ideology, but that point of view seems to be an endangered species in 2010.
Over the last 25 years what is known as the "social gradient" has been described by careful population research. This means that your position on the socioeconomic scale or social hierarchy will have a profound effect on your health. This is true even if we control for lifestyle(e.g smoking, obesity) and access to health care. People at the highest level of education, income, and social standing have the highest degree of health status. Those a notch lower have a little bit poorer health status, and so on down to the lowest levels of society, in which people have by far the poorest health status.
It can be argued that social determination of your health is inherently unfair. However, most people are apathetic because it seems so hopeless, as a practical matter to contemplate eliminating poverty or substandard housing. We know how to do these things in principle, but have had little success with real people in real communities.
This is certainly in the mainstream of progressive ideology, but that point of view seems to be an endangered species in 2010.
Wednesday, July 7, 2010
Survival of the Fittest , part 3
There is a process of natural selection going on with insects, weeds, and microorganisms, and each of these have major implications for human welfare. Since the development of chemical controls for each organism(insecticides, herbicides, and antibiotics), survivors able to resist the impact of those controls have prospered. The population of chemical-resistant insects, weeds and microorganisms has been steadily growing, presenting a truly threatening future unless new technology comes along. Out of control insects spread infectious disease. Out of control weeds threaten our food production, and out of control microorganisms present a scenario where we run out of effective antibiotics, and more and more infections are untreatable. The world has faced similar threats in the past, and we have always been able to adapt and overcome. Time will tell whether this is the case with these current threats.
Tuesday, July 6, 2010
Survival of the Fittest, part 2
While humans are generally protected from the most severe consequences of natural selection, there are some exhibits of survival of the fittest. It is generally recognized that African peoples with the sickle cell trait are resistant to the ravages of malaria. On the other hand, children with juvenile diabetes should be at a disadvantage; without modern treatment methods, these children would die before being able to produce children. In that case, over a number of generations, the juvenile diabetes trait should die out, as only children without that genetic trait would reproduce.
Of course, natural selection and survival of the fittest is not only experienced by humans, but by other organisms. Natural selection in other organisms can effect humans as well.
To be continued.
Of course, natural selection and survival of the fittest is not only experienced by humans, but by other organisms. Natural selection in other organisms can effect humans as well.
To be continued.
Friday, July 2, 2010
Survival of the Fittest
In the natural world we see adaptation of living things to changes and challenges in the environment. Those organisms which, for whatever reason, are able to overcome the threat or exploit the opportunity provided by the change will thrive, whereas those organisms less able to do so will decline, die, or assume a lower rung on the natural pecking order. As humans we are cushioned against the harsh reality of "natural selection" because our intelligence makes it possible to cope and adopt more creatively and successfully, but also because our life cycles are long enough that it is rare that our generation cycles make possible a culling of the race. While the body of knowledge possessed by humans has grown exponentially, and the average person in 2010 has more information, there is no evidence that the proportion of people with high IQ has changed. Natural selection would suggest that smart people would have greater capability to survive while those of lower intelligence would be relatively less likely to survive, and that over time, average intelligence would rise on the IQ scale. This has not happened, for many reasons.
These thoughts will make their way around to health promotion applications. To be continued.
These thoughts will make their way around to health promotion applications. To be continued.
Subscribe to:
Comments (Atom)